You Might Have Fallen Arches?
Overview
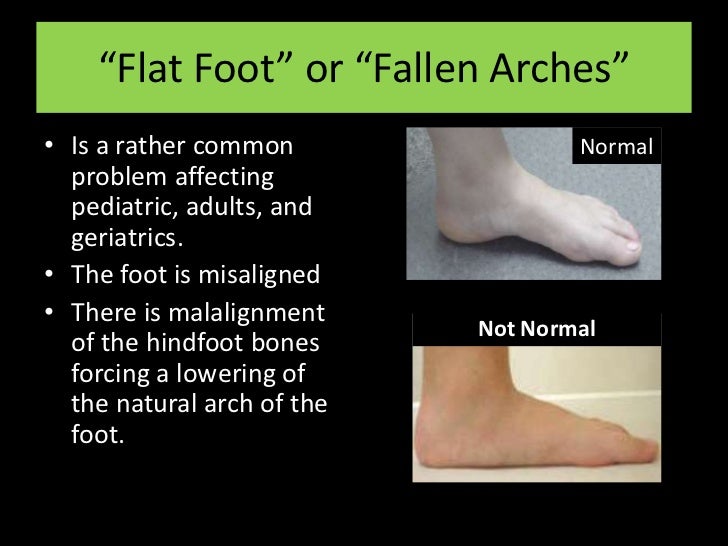
The term 'fallen arches' is rather a historical one, but is one many people seem to have heard of. What it essentially refers to is a ligament problem in the sole of his foot where these run along its length. In most people these ligaments provide support to the foot when walking and help keep the foot in a normal anatomical position. Some people however seem to have laxity in these ligaments so the foot becomes under undue strain and pain can occur as a result.
Causes
Infants and young children naturally have flat feet. The arch should develop over time. Sometimes, the arch does not develop. It is not always clear why this happens. Flat feet may develop because of ruptured or damaged tendon that supports the arch, medical conditions that affect muscles or nerves in the foot, degenerative changes in certain foot joints, Ligament damage in the foot.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms below. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
People who have flat feet without signs or symptoms that bother them do not generally have to see a doctor or podiatrist about them. However, if any of the following occur, you should see your GP or a podiatrist. The fallen arches (flat feet) have developed recently. You experience pain in your feet, ankles or lower limbs. Your unpleasant symptoms do not improve with supportive, well-fitted shoes. Either or both feet are becoming flatter. Your feet feel rigid (stiff). Your feet feel heavy and unwieldy. Most qualified health care professionals can diagnose flat feet just by watching the patient stand, walk and examining his/her feet. A doctor will also look at the patient's medical history. The feet will be observed from the front and back. The patient may be asked to stand on tip-toe while the doctor examines the shape and functioning of each foot. In some cases the physician may order an X-ray, CT (computed tomography) scan, or MRI (magnetic resonance imaging) scan.
What is PES Planovalgus deformity?
Non Surgical Treatment
Most flexible flat feet are asymptomatic, and do not cause pain. In these cases, there is usually no cause for concern, and the condition may be considered a normal human variant. Flat feet were formerly a physical-health reason for service-rejection in many militaries. However, three military studies on asymptomatic adults (see section below), suggest that persons with asymptomatic flat feet are at least as tolerant of foot stress as the population with various grades of arch. Asymptomatic flat feet are no longer a service disqualification in the U.S. military.
Surgical Treatment

Generally one of the following procedures is used to surgically repair a flat foot or fallen arch. Arthrodesis. One or more of your bones in the foot or ankle are fused together. Osteotomy. Correcting alignment by cutting and reshaping a bone. Excision. Removing a bone or a bone spur. Synovectomy. Cleaning the sheath that covers the tendon. Tendon transfer. Using a piece of one tendon to lengthen or replace another. Arthroereisis. placing a small device in the subtalar joint to limit motion. For most people, treatment is successful, regardless of the cause, although the cause does does play a major role in determining your prognosis. Some causes do not need treatment, while others require a surgical fix.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
The term 'fallen arches' is rather a historical one, but is one many people seem to have heard of. What it essentially refers to is a ligament problem in the sole of his foot where these run along its length. In most people these ligaments provide support to the foot when walking and help keep the foot in a normal anatomical position. Some people however seem to have laxity in these ligaments so the foot becomes under undue strain and pain can occur as a result.
Causes
Infants and young children naturally have flat feet. The arch should develop over time. Sometimes, the arch does not develop. It is not always clear why this happens. Flat feet may develop because of ruptured or damaged tendon that supports the arch, medical conditions that affect muscles or nerves in the foot, degenerative changes in certain foot joints, Ligament damage in the foot.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms below. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
People who have flat feet without signs or symptoms that bother them do not generally have to see a doctor or podiatrist about them. However, if any of the following occur, you should see your GP or a podiatrist. The fallen arches (flat feet) have developed recently. You experience pain in your feet, ankles or lower limbs. Your unpleasant symptoms do not improve with supportive, well-fitted shoes. Either or both feet are becoming flatter. Your feet feel rigid (stiff). Your feet feel heavy and unwieldy. Most qualified health care professionals can diagnose flat feet just by watching the patient stand, walk and examining his/her feet. A doctor will also look at the patient's medical history. The feet will be observed from the front and back. The patient may be asked to stand on tip-toe while the doctor examines the shape and functioning of each foot. In some cases the physician may order an X-ray, CT (computed tomography) scan, or MRI (magnetic resonance imaging) scan.
What is PES Planovalgus deformity?
Non Surgical Treatment
Most flexible flat feet are asymptomatic, and do not cause pain. In these cases, there is usually no cause for concern, and the condition may be considered a normal human variant. Flat feet were formerly a physical-health reason for service-rejection in many militaries. However, three military studies on asymptomatic adults (see section below), suggest that persons with asymptomatic flat feet are at least as tolerant of foot stress as the population with various grades of arch. Asymptomatic flat feet are no longer a service disqualification in the U.S. military.
Surgical Treatment
Generally one of the following procedures is used to surgically repair a flat foot or fallen arch. Arthrodesis. One or more of your bones in the foot or ankle are fused together. Osteotomy. Correcting alignment by cutting and reshaping a bone. Excision. Removing a bone or a bone spur. Synovectomy. Cleaning the sheath that covers the tendon. Tendon transfer. Using a piece of one tendon to lengthen or replace another. Arthroereisis. placing a small device in the subtalar joint to limit motion. For most people, treatment is successful, regardless of the cause, although the cause does does play a major role in determining your prognosis. Some causes do not need treatment, while others require a surgical fix.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Best Heel Lifts For Leg Length Discrepancy
Overview
Leg length discrepancy, or as it has been alternatively termed, the short leg syndrome, is by far the most important postural asymmetry. Limb length discrepancy is simply defined as a condition where one leg is shorter than the other. If a substantial difference exists, disruptive effects on gait and posture can occur. Leg length discrepancy can be divided into two etiological groups. Structural. True shortening of the skeleton from congenital, traumatic or diseased origins. Functional. Development from altered mechanics of the lower body, such as foot hyperpronation or supination, pelvic obliquity, muscle/joint imbalances, poor trunk stabilization and deep fascial strain patterns.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.

increase height quickly
Surgical Treatment
Surgeries for LLD are designed to do one of three general things ? shorten the long leg, stop or slow the growth of the longer or more rapidly growing leg, or lengthen the short leg. Stopping the growth of the longer leg is the most commonly utilized of the three approaches and involves an operation known as an epiphysiodesis , in which the growth plate of either the lower femur or upper tibia is visualized in the operating room using fluoroscopy (a type of real-time radiographic imaging) and ablated , which involves drilling into the region several times, such that the tissue is no longer capable of bone growth. Because the epiphyseal growth capabilities cannot be restored following the surgery, proper timing is crucial. Usually the operation is planned for the last 2 to 3 years of growth and has excellent results, with children leaving the hospital within a few days with good mobility. However, it is only appropriate for LLD of under 5cm.
Leg length discrepancy, or as it has been alternatively termed, the short leg syndrome, is by far the most important postural asymmetry. Limb length discrepancy is simply defined as a condition where one leg is shorter than the other. If a substantial difference exists, disruptive effects on gait and posture can occur. Leg length discrepancy can be divided into two etiological groups. Structural. True shortening of the skeleton from congenital, traumatic or diseased origins. Functional. Development from altered mechanics of the lower body, such as foot hyperpronation or supination, pelvic obliquity, muscle/joint imbalances, poor trunk stabilization and deep fascial strain patterns.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.
increase height quickly
Surgical Treatment
Surgeries for LLD are designed to do one of three general things ? shorten the long leg, stop or slow the growth of the longer or more rapidly growing leg, or lengthen the short leg. Stopping the growth of the longer leg is the most commonly utilized of the three approaches and involves an operation known as an epiphysiodesis , in which the growth plate of either the lower femur or upper tibia is visualized in the operating room using fluoroscopy (a type of real-time radiographic imaging) and ablated , which involves drilling into the region several times, such that the tissue is no longer capable of bone growth. Because the epiphyseal growth capabilities cannot be restored following the surgery, proper timing is crucial. Usually the operation is planned for the last 2 to 3 years of growth and has excellent results, with children leaving the hospital within a few days with good mobility. However, it is only appropriate for LLD of under 5cm.
What Can Cause Heel Aches
Overview

Pain arises in the centre of the heel and sometimes can spread to the arch region of the foot. Some patients complain of intense pain when walking the first few steps in the morning and after periods of rest. The most common cause of heel pain is plantar fascitis. The plantar fascia is a broad band of tissue that runs along the bottom of the foot. When this band of tissue is damaged due to biomechanical reasons or inappropriate running shoes then the tissue can become inflamed or even tear at the heel bone. This can be very painful.
Causes
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis. An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
Depending on the condition, the cause of heel pain is diagnosed using a number of tests, including medical history, physical examination, including examination of joints and muscles of the foot and leg, X-rays.
Non Surgical Treatment
Most patients get better with the help of nonsurgical treatments. Stretches for the calf muscles on the back of the lower leg take tension off the plantar fascia. A night splint can be worn while you sleep. The night splint keeps your foot from bending downward. It places a mild stretch on the calf muscles and the plantar fascia. Some people seem to get better faster when using a night splint. They report having less heel pain when placing the sore foot on the ground in the morning. There have been a few studies that reported no significant benefit from adding night splinting to a program of antiinflammatory meds and stretching. Other studies report the benefits of short-term casting to unload the heel, immobilize the plantar fascia, and reduce repetitive microtrauma. Supporting the arch with a well fitted arch support, or orthotic, may also help reduce pressure on the plantar fascia. Placing a special type of insert into the shoe, called a heel cup, can reduce the pressure on the sore area. Wearing a silicone heel pad adds cushion to a heel that has lost some of the fat pad through degeneration. Shock wave therapy is a newer form of nonsurgical treatment. It uses a machine to generate shock wave pulses to the sore area. Patients generally receive the treatment once each week for up to three weeks. It is not known exactly why it works for plantar fasciitis. It's possible that the shock waves disrupt the plantar fascial tissue enough to start a healing response. The resulting release of local growth factors and stem cells causes an increase in blood flow to the area. Recent studies indicate that this form of treatment can help ease pain, while improving range of motion and function.
Surgical Treatment
Only a relatively few cases of heel pain require surgery. If required, surgery is usually for the removal of a spur, but also may involve release of the plantar fascia, removal of a bursa, or a removal of a neuroma or other soft-tissue growth.
hold loose high heeled shoes
Prevention

Heel pain is commonly caused from shoes that do not fit properly. In addition, shoes need to have ample cushioning and support, particularly through the heel, ball of the foot, and arch. Shoes should also be replaced if they become too worn. One sure sign of wear and tear is overly worn areas of a shoe's insoles. If the heel or ball of the foot is particularly worn, damage could easily occur since the bottom of the foot is not getting the cushioning it needs.
Pain arises in the centre of the heel and sometimes can spread to the arch region of the foot. Some patients complain of intense pain when walking the first few steps in the morning and after periods of rest. The most common cause of heel pain is plantar fascitis. The plantar fascia is a broad band of tissue that runs along the bottom of the foot. When this band of tissue is damaged due to biomechanical reasons or inappropriate running shoes then the tissue can become inflamed or even tear at the heel bone. This can be very painful.
Causes
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis. An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
Depending on the condition, the cause of heel pain is diagnosed using a number of tests, including medical history, physical examination, including examination of joints and muscles of the foot and leg, X-rays.
Non Surgical Treatment
Most patients get better with the help of nonsurgical treatments. Stretches for the calf muscles on the back of the lower leg take tension off the plantar fascia. A night splint can be worn while you sleep. The night splint keeps your foot from bending downward. It places a mild stretch on the calf muscles and the plantar fascia. Some people seem to get better faster when using a night splint. They report having less heel pain when placing the sore foot on the ground in the morning. There have been a few studies that reported no significant benefit from adding night splinting to a program of antiinflammatory meds and stretching. Other studies report the benefits of short-term casting to unload the heel, immobilize the plantar fascia, and reduce repetitive microtrauma. Supporting the arch with a well fitted arch support, or orthotic, may also help reduce pressure on the plantar fascia. Placing a special type of insert into the shoe, called a heel cup, can reduce the pressure on the sore area. Wearing a silicone heel pad adds cushion to a heel that has lost some of the fat pad through degeneration. Shock wave therapy is a newer form of nonsurgical treatment. It uses a machine to generate shock wave pulses to the sore area. Patients generally receive the treatment once each week for up to three weeks. It is not known exactly why it works for plantar fasciitis. It's possible that the shock waves disrupt the plantar fascial tissue enough to start a healing response. The resulting release of local growth factors and stem cells causes an increase in blood flow to the area. Recent studies indicate that this form of treatment can help ease pain, while improving range of motion and function.
Surgical Treatment
Only a relatively few cases of heel pain require surgery. If required, surgery is usually for the removal of a spur, but also may involve release of the plantar fascia, removal of a bursa, or a removal of a neuroma or other soft-tissue growth.
hold loose high heeled shoes
Prevention
Heel pain is commonly caused from shoes that do not fit properly. In addition, shoes need to have ample cushioning and support, particularly through the heel, ball of the foot, and arch. Shoes should also be replaced if they become too worn. One sure sign of wear and tear is overly worn areas of a shoe's insoles. If the heel or ball of the foot is particularly worn, damage could easily occur since the bottom of the foot is not getting the cushioning it needs.
How To Estimate Leg Length Discrepancy At Home
Overview
Some people have an ?apparent? LLD which may make the affected leg seem longer than the other leg. There are several factors that can contribute to this feeling. Most commonly, contractures or shortening of the muscles surrounding the hip joint and pelvis make the involved leg feel longer, even when both legs are really the same length. Additionally, contractures of the muscles around the lower back from spinal disorders (i.e. arthritis, spinal stenosis), curvatures of the spine from scoliosis, and deformities of the knee or ankle joint can make one leg seem longer or shorter. In the general public, some people have an ?apparent LLD? as long as one half inch but usually don?t notice it because the LLD occurs over time. A ?true? LLD is where one leg is actually longer than the other. Patients can have unequal leg lengths of 1/4? to 1/2? and never feel it too! You can also have combinations of ?True? and ?Apparent? LLDs. During total hip replacement surgery, the surgeon may ?lengthen? the involved leg by stretching the muscles and ligaments that were contracted, as well as by restoring the joint space that had become narrowed from the arthritis. This is usually a necessary part of the surgery because it also provides stability to the new hip joint. Your surgeon takes measurements of your leg lengths on x-ray prior to surgery. Your surgeon always aims for equal leg lengths if at all possible and measures the length of your legs before and during surgery in order to achieve this goal. Occasionally, surgeons may need to lengthen the operable leg to help improve stability and prevent dislocations as well improve the muscle function around the hip.
Causes
Common causes include bone infection, bone diseases, previous injuries, or broken bones. Other causes may include birth defects, arthritis where there is a loss of articular surface, or neurological conditions.
Symptoms
Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
Treatment for an LLD depends on the amount of difference and the cause, if known. The doctor will discuss treatment options carefully with you and your child before any decisions are made. It is important to note that treatment is planned with the child?s final height and leg lengths in mind, not the current leg lengths. Treatment is generally not needed if the child?s final LLD is predicted to be 2 centimeters or less at full height. However, the child should return to an orthopaedic doctor by age 10 for re-evaluation. Treatment is often recommended for LLDs predicted to be more than 2 centimeters at full height. If treatment is done, it usually doesn?t begin until the child starts walking. Possible treatment options include, A ?lift? in one shoe to level the child?s hips. This is often the only treatment needed for small discrepancies.

how to increase height naturally after 21
Surgical Treatment
Surgical options in leg length discrepancy treatment include procedures to lengthen the shorter leg, or shorten the longer leg. Your child's physician will choose the safest and most effective method based on the aforementioned factors. No matter the surgical procedure performed, physical therapy will be required after surgery in order to stretch muscles and help support the flexibility of the surrounding joints. Surgical shortening is safer than surgical lengthening and has fewer complications. Surgical procedures to shorten one leg include removing part of a bone, called a bone resection. They can also include epiphysiodesis or epiphyseal stapling, where the growth plate in a bone is tethered or stapled. This slows the rate of growth in the surgical leg.
Some people have an ?apparent? LLD which may make the affected leg seem longer than the other leg. There are several factors that can contribute to this feeling. Most commonly, contractures or shortening of the muscles surrounding the hip joint and pelvis make the involved leg feel longer, even when both legs are really the same length. Additionally, contractures of the muscles around the lower back from spinal disorders (i.e. arthritis, spinal stenosis), curvatures of the spine from scoliosis, and deformities of the knee or ankle joint can make one leg seem longer or shorter. In the general public, some people have an ?apparent LLD? as long as one half inch but usually don?t notice it because the LLD occurs over time. A ?true? LLD is where one leg is actually longer than the other. Patients can have unequal leg lengths of 1/4? to 1/2? and never feel it too! You can also have combinations of ?True? and ?Apparent? LLDs. During total hip replacement surgery, the surgeon may ?lengthen? the involved leg by stretching the muscles and ligaments that were contracted, as well as by restoring the joint space that had become narrowed from the arthritis. This is usually a necessary part of the surgery because it also provides stability to the new hip joint. Your surgeon takes measurements of your leg lengths on x-ray prior to surgery. Your surgeon always aims for equal leg lengths if at all possible and measures the length of your legs before and during surgery in order to achieve this goal. Occasionally, surgeons may need to lengthen the operable leg to help improve stability and prevent dislocations as well improve the muscle function around the hip.
Causes
Common causes include bone infection, bone diseases, previous injuries, or broken bones. Other causes may include birth defects, arthritis where there is a loss of articular surface, or neurological conditions.
Symptoms
Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
Treatment for an LLD depends on the amount of difference and the cause, if known. The doctor will discuss treatment options carefully with you and your child before any decisions are made. It is important to note that treatment is planned with the child?s final height and leg lengths in mind, not the current leg lengths. Treatment is generally not needed if the child?s final LLD is predicted to be 2 centimeters or less at full height. However, the child should return to an orthopaedic doctor by age 10 for re-evaluation. Treatment is often recommended for LLDs predicted to be more than 2 centimeters at full height. If treatment is done, it usually doesn?t begin until the child starts walking. Possible treatment options include, A ?lift? in one shoe to level the child?s hips. This is often the only treatment needed for small discrepancies.
how to increase height naturally after 21
Surgical Treatment
Surgical options in leg length discrepancy treatment include procedures to lengthen the shorter leg, or shorten the longer leg. Your child's physician will choose the safest and most effective method based on the aforementioned factors. No matter the surgical procedure performed, physical therapy will be required after surgery in order to stretch muscles and help support the flexibility of the surrounding joints. Surgical shortening is safer than surgical lengthening and has fewer complications. Surgical procedures to shorten one leg include removing part of a bone, called a bone resection. They can also include epiphysiodesis or epiphyseal stapling, where the growth plate in a bone is tethered or stapled. This slows the rate of growth in the surgical leg.
Coping with Mortons Neuroma
Overview
 Morton's neuroma is a condition that affects one of the nerves that run between the long bones (metatarsals) in the foot. The exact cause is not certain. Symptoms include pain, burning, numbness and tingling between two of the toes of the foot. About a quarter of people just need simple treatments including modification of their footwear. Sometimes surgery is needed for long-standing (chronic) symptoms.
Morton's neuroma is a condition that affects one of the nerves that run between the long bones (metatarsals) in the foot. The exact cause is not certain. Symptoms include pain, burning, numbness and tingling between two of the toes of the foot. About a quarter of people just need simple treatments including modification of their footwear. Sometimes surgery is needed for long-standing (chronic) symptoms.
Causes
A Morton's neuroma commonly occurs due to repetitive weight bearing activity (such as walking or running) particularly when combined with tight fitting shoes or excessive pronation of the feet (i.e. "flat-feet"). The condition is also more common in patients with an unstable forefoot allowing excessive movement between the metatarsal bones. A Morton's neuroma can also occur due to certain foot deformities, trauma to the foot, or the presence of a ganglion or inflamed bursa in the region which may place compressive forces on the nerve.
Symptoms
The primary symptoms include sharp, shooting pain, numbness or paresthesia in the forefoot and extending distally into the toes, typically in the region of the third and fourth toes. Symptoms are aggravated with narrow toe box shoes or those with high heels. There is usually a reduction of symptoms when walking barefoot or wearing shoes with an appropriately wide toe box. Symptoms are also aggravated with shoes that are tied too tight.
Diagnosis
Diagnosis of Morton?s Neuroma typically involves a physical examination of the affected foot. Your health care provider will ask you about your symptoms and examine your feet and toes. He will manipulate your toes, pushing them from side to side and squeezing on the spaces in between. This physical exam will allow your health care provider to feel for any lumps that may be present under the soft tissue of your feet. Your health care provider may also listen for any clicking sounds that your bones may be making. Known as Muldor?s Sign, this clicking is common amongst sufferers of foot neuroma. Occasionally, an x-ray or MRI (magnetic resonance imaging) is performed to help rule out any breaks, sprains, or fractures in your foot.
Non Surgical Treatment
It can be helpful to perform deep stripping massage techniques along the length of the tibial nerve and the medial and lateral plantar nerves. After properly mobilizing these tissues, moving the foot and toes through a full range of motion to make sure the nerve can move freely will also be helpful. Foot pain like that occurring in Morton's neuroma, can become a debilitating and painful condition. And while massage can be helpful for this condition, it is also clear that improperly applied massage can aggravate it and make it worse. Consequently it is crucial that we use good clinical reasoning and appropriate evaluation methods to most effectively help these clients.
Surgical Treatment
For those who are suffering severely with Morton?s Neuroma, surgery is a possibility. An orthopedic surgeon can remove the growth and repair your foot relatively easily. However, Morton?s Neuroma surgery is associated with a lengthy recovery time and there is a possibility that the neuroma may return.
Morton's neuroma is a condition that affects one of the nerves that run between the long bones (metatarsals) in the foot. The exact cause is not certain. Symptoms include pain, burning, numbness and tingling between two of the toes of the foot. About a quarter of people just need simple treatments including modification of their footwear. Sometimes surgery is needed for long-standing (chronic) symptoms.Causes
A Morton's neuroma commonly occurs due to repetitive weight bearing activity (such as walking or running) particularly when combined with tight fitting shoes or excessive pronation of the feet (i.e. "flat-feet"). The condition is also more common in patients with an unstable forefoot allowing excessive movement between the metatarsal bones. A Morton's neuroma can also occur due to certain foot deformities, trauma to the foot, or the presence of a ganglion or inflamed bursa in the region which may place compressive forces on the nerve.
Symptoms
The primary symptoms include sharp, shooting pain, numbness or paresthesia in the forefoot and extending distally into the toes, typically in the region of the third and fourth toes. Symptoms are aggravated with narrow toe box shoes or those with high heels. There is usually a reduction of symptoms when walking barefoot or wearing shoes with an appropriately wide toe box. Symptoms are also aggravated with shoes that are tied too tight.
Diagnosis
Diagnosis of Morton?s Neuroma typically involves a physical examination of the affected foot. Your health care provider will ask you about your symptoms and examine your feet and toes. He will manipulate your toes, pushing them from side to side and squeezing on the spaces in between. This physical exam will allow your health care provider to feel for any lumps that may be present under the soft tissue of your feet. Your health care provider may also listen for any clicking sounds that your bones may be making. Known as Muldor?s Sign, this clicking is common amongst sufferers of foot neuroma. Occasionally, an x-ray or MRI (magnetic resonance imaging) is performed to help rule out any breaks, sprains, or fractures in your foot.
Non Surgical Treatment
It can be helpful to perform deep stripping massage techniques along the length of the tibial nerve and the medial and lateral plantar nerves. After properly mobilizing these tissues, moving the foot and toes through a full range of motion to make sure the nerve can move freely will also be helpful. Foot pain like that occurring in Morton's neuroma, can become a debilitating and painful condition. And while massage can be helpful for this condition, it is also clear that improperly applied massage can aggravate it and make it worse. Consequently it is crucial that we use good clinical reasoning and appropriate evaluation methods to most effectively help these clients.
Surgical Treatment
For those who are suffering severely with Morton?s Neuroma, surgery is a possibility. An orthopedic surgeon can remove the growth and repair your foot relatively easily. However, Morton?s Neuroma surgery is associated with a lengthy recovery time and there is a possibility that the neuroma may return.
For Leg Length Discrepancy Chiropodists Prefer Shoe Lifts
There are not one but two unique variations of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is structurally shorter than the other. As a result of developmental phases of aging, the human brain picks up on the walking pattern and recognizes some variation. The body usually adapts by dipping one shoulder over to the "short" side. A difference of less than a quarter inch isn't very excessive, demand Shoe Lifts to compensate and in most cases won't have a profound effect over a lifetime.

Leg length inequality goes typically undiagnosed on a daily basis, yet this condition is simply remedied, and can reduce many cases of chronic back pain.
Therapy for leg length inequality typically consists of Shoe Lifts. They are cost-effective, usually priced at under twenty dollars, in comparison to a custom orthotic of $200 if not more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is easily the most common ailment afflicting people today. Around 80 million men and women suffer from back pain at some stage in their life. It's a problem that costs companies huge amounts of money each year due to lost time and productivity. Fresh and better treatment solutions are constantly sought after in the hope of minimizing the economical impact this condition causes.

Men and women from all corners of the world suffer from foot ache due to leg length discrepancy. In a lot of these situations Shoe Lifts can be of beneficial. The lifts are capable of relieving any pain and discomfort in the feet. Shoe Lifts are recommended by countless experienced orthopaedic doctors.
In order to support the human body in a well-balanced fashion, the feet have a critical part to play. In spite of that, it is sometimes the most overlooked zone in the body. Many people have flat-feet meaning there is unequal force exerted on the feet. This will cause other parts of the body such as knees, ankles and backs to be impacted too. Shoe Lifts guarantee that the right posture and balance are restored.
Leg length inequality goes typically undiagnosed on a daily basis, yet this condition is simply remedied, and can reduce many cases of chronic back pain.
Therapy for leg length inequality typically consists of Shoe Lifts. They are cost-effective, usually priced at under twenty dollars, in comparison to a custom orthotic of $200 if not more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is easily the most common ailment afflicting people today. Around 80 million men and women suffer from back pain at some stage in their life. It's a problem that costs companies huge amounts of money each year due to lost time and productivity. Fresh and better treatment solutions are constantly sought after in the hope of minimizing the economical impact this condition causes.
Men and women from all corners of the world suffer from foot ache due to leg length discrepancy. In a lot of these situations Shoe Lifts can be of beneficial. The lifts are capable of relieving any pain and discomfort in the feet. Shoe Lifts are recommended by countless experienced orthopaedic doctors.
In order to support the human body in a well-balanced fashion, the feet have a critical part to play. In spite of that, it is sometimes the most overlooked zone in the body. Many people have flat-feet meaning there is unequal force exerted on the feet. This will cause other parts of the body such as knees, ankles and backs to be impacted too. Shoe Lifts guarantee that the right posture and balance are restored.
Is A Hammer Toe Uncomfortable
 Overview
Overview
Hammertoes are quite common and may range from mild to severe. A Hammer toe is a contracture, or bending, of one or more toes, usually due to an imbalance between the muscles or tendons on the top and bottom of the toes. Over time, the affected toes lose flexibility, becoming rigid Hammer toe and fixed in a contracted position. The abnormal bend positions the knuckle of the toe upward, causing it to push against the top of the shoe leading to additional problems. The condition usually becomes progressively worse if not treated.
Causes
Hammer toe results from shoes that don't fit properly or a muscle imbalance, usually in combination with one or more other factors. Muscles work in pairs to straighten and bend the toes. If the toe is bent and held in one position long enough, the muscles tighten and cannot stretch out. Shoes that narrow toward the toe may make your forefoot look smaller. But they also push the smaller toes into a flexed (bent) position. The toes rub against the shoe, leading to the formation of corns and calluses, which further aggravate the condition. A higher heel forces the foot down and squishes the toes against the shoe, increasing the pressure and the bend in the toe. Eventually, the toe muscles become unable to straighten the toe, even when there is no confining shoe.
 Symptoms
Symptoms
Patients with hammer toe(s) may develop pain on the top of the toe(s), tip of the toe, and/or on the ball of the foot. Excessive pressure from shoes may result in the formation of a hardened portion of skin (corn or callus) on the knuckle and/or ball of the foot. Some people may not recognize that they have a hammer toe, rather they identity the excess skin build-up of a corn.The toe(s) may become irritated, red, warm, and/or swollen. The pain may be dull and mild or severe and sharp. Pain is often made worse by shoes, especially shoes that crowd the toes. While some hammer toes may result in significant pain, others may not be painful at all. Painful toes can prevent you from wearing stylish shoes.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. If the deformed toe is very painful, your doctor may recommend that you have a fluid sample withdrawn from the joint with a needle so the fluid can be checked for signs of infection or gout (arthritis from crystal deposits).
Non Surgical Treatment
Try to find shoes that are soft, roomy, and comfortable and avoid tight shoes or shoes with high heels. A shoe repair shop may be able to stretch a small pocket in regular shoes to make room for the hammertoe. Have a professional pedicure. Sometimes a skilled manicurist can file down a painful corn. Follow your healthcare provider's instructions. Ask your provider what activities you should avoid and when you can return to your normal activities, how to take care of yourself at home, what symptoms or problems you should watch for and what to do if you have them. Make sure you know when you should come back for a checkup.
Surgical Treatment
Joint resection procedures involves removing part of one of the two small joints of the toe directly underneath where the digit is crooked. The purpose is to make room for the toe to be re-positioned flat or straight. Because hammer toes become rigid or fixed with time, removing the joint becomes the only option when the knuckle is stiff. Its important to understand that this procedure does not involve the joint of the ball of the foot, rather the a small joint of the toe. Medical terminology for this procedure is called a proximal interphalangeal joint arthroplasty or a distal interphalangeal joint arthroplasty, with the latter involving the joint closer to the tip of the toe.